IR Information
FAQ
Company Profile
- What is the origin of the company name?
-
Our founder is a nephrologist, and when we first started, there were very few drugs to treat kidney disease. Our company was founded with the goal of developing drugs to treat kidney disease, so we named it Renascience, which means “science of kidneys.” Renascience also has the meaning of “renascence.”
Drug development is not always being done in areas where it is needed, and drug development is lagging behind in areas where it is difficult to develop, such as kidney disease (where efficacy evaluation is difficult to carry out because it takes time) and rare diseases (diseases with few patients and low sales). Therefore, we are currently actively working on drug development in areas where it is difficult to develop and rare diseases.
- What are the reasons for developing various modalities (therapeutic technologies)?
-
Our goal is to create new medical treatments that will solve medical issues and allow people to enjoy lifelong health, both physically and mentally. We are not a venture specializing in a specific technology, so we are not concerned with modality.
The pharmaceutical industry is diversifying from development centered on small molecule drugs to biopharmaceuticals. Furthermore, with recent advances in engineering and information technology, the search for new medical treatments that combine information and engineering technology is also progressing, and major pharmaceutical companies in Europe, the United States, and Japan have already shifted from pharmaceutical-only businesses to businesses that cover medical solutions in general. Medical treatment options are also expanding, including pharmaceuticals, medical devices, and even program medical devices and apps that utilize artificial intelligence (AI).
To that end, in addition to the chemical and biological research that has been our main focus thus far, we would like to broaden our horizons to include engineering and information research, creating a diverse and attractive research and business portfolio.
- What medical issues are you working on?
-
The World Health Organization (WHO) classifies major diseases associated with aging and lifestyle—known as age-related diseases—as “non-communicable diseases” (NCDs), specifically targeting cancer, diabetes, respiratory diseases, and cardiovascular diseases. It is estimated that these four conditions account for 70–80% of deaths worldwide. Our product development pipeline targets all four of these disease categories.
The World Health Organization (WHO) classifies major diseases associated with aging and lifestyle—known as age-related diseases—as “non-communicable diseases” (NCDs), specifically targeting cancer, diabetes, respiratory diseases, and cardiovascular diseases. It is estimated that these four conditions account for 70–80% of deaths worldwide. Our product development pipeline targets all four of these disease categories.
- What are the advantages of the open innovation?
-
Pharmaceutical development is a field characterized by high R&D risk, as it entails low success rates, long development timelines, and substantial investment. Consequently, mitigating risk by building a portfolio that combines multiple development pipelines is crucial. Recent trends in medical innovation highlight the importance of leveraging cutting-edge technologies and drug discovery leads from research institutions—such as universities—as well as clinical data and insights from actual medical practice.
We actively promote collaborations with universities and medical institutions, establishing an open-innovation R&D model that utilizes external expertise, technology, and data. Furthermore, we provide our proprietary compounds to researchers as open resources; this enables them to pursue new research themes and—following patent applications—engage in activities such as conference presentations, academic publications, and grant applications. Through such collaborations, we incorporate diverse insights and drive the creation of new drug discovery leads.
Leveraging these external resources allows us to efficiently advance multiple pipelines and mitigate R&D risk—even with limited human and financial resources—compared to the alternative of building all development capabilities in-house.
We are driving efficient innovation through partnerships and collaborations with universities, various companies, and research institutions.
- Why did you establish the Tohoku University Renascience Open Innovation Labo (TREx) and Hiroshima University Renascience Open Innovation Labo (HiREx)?
-
In January 2022, we opened the Tohoku University Renascience Open Innovation Lab (Tohoku University x Renascience = TREx) at the Medicinal Hub of the Tohoku University Graduate School of Medicine (2-1 Seiryou-cho, Aoba-ku, Sendai, Miyagi Prefecture, Faculty of Medicine Building No. 5).
When our company was founded, we had a research institute in the Kawasaki Bio Special Zone in Kanagawa Prefecture, which included a facility for breeding animal models of kidney disease. Later, as our research subjects expanded from kidney disease to many other disease areas and the research stage progressed from basic research to clinical trials, we closed our original research institute, which focused on animal models of kidney disease.
However, we felt that there was a need for a place where cutting-edge scientific and technological achievements could be utilized in many disease areas, a place for face-to-face interaction with doctors and researchers, and a place for open innovation with government agencies and medical industry companies, and so we decided to open TREx.
Pharmaceutical development is a field characterized by high R&D risk, as it entails low success rates, long development timelines, and substantial investment. Consequently, mitigating risk by building a portfolio that combines multiple development pipelines is crucial. Recent trends in medical innovation highlight the importance of leveraging cutting-edge technologies and drug discovery leads from research institutions—such as universities—as well as clinical data and insights from actual medical practice.
We actively promote collaborations with universities and medical institutions, establishing an open-innovation R&D model that utilizes external expertise, technology, and data. Furthermore, we provide our proprietary compounds to researchers as open resources; this enables them to pursue new research themes and—following patent applications—engage in activities such as conference presentations, academic publications, and grant applications. Through such collaborations, we incorporate diverse insights and drive the creation of new drug discovery leads.
Leveraging these external resources allows us to efficiently advance multiple pipelines and mitigate R&D risk—even with limited human and financial resources—compared to the alternative of building all development capabilities in-house.
We are driving efficient innovation through partnerships and collaborations with universities, various companies, and research institutions.
TREx is also the first base location based on the Agreement on Regional Economic Development between Sendai City and Tohoku University, which was concluded in April 2021.
At TREx, 1) collaboration with different industries such as researchers at the Tohoku University Graduate School of Medicine, doctors at Tohoku University Hospital, companies participating in the Medicinal Hub, and government agencies has been accelerated, 2) research in the existing development pipeline has been promoted and multiple new seeds have been introduced, 3) investigator-initiated clinical trials, medical data acquisition, public funding, and approval strategy planning can be carried out efficiently and quickly, and 4) it has also led to the development and retention of human resources. This has allowed us to further accelerate the high efficiency of research and development, which is one of our strengths.
In April 2023, we signed a comprehensive collaboration agreement with Hiroshima University, and following TREx, we opened the Hiroshima University Renascience Open Innovation Lab (Hiroshima University x Renascience = HiREx). Using HiREx, we are conducting multiple clinical trials, including investigator-initiated clinical trials of pharmaceuticals for non-small cell lung cancer and cutaneous angiosarcoma, and clinical performance tests of programmable medical devices such as AI to support diabetes treatment and AI to support maintenance hemodialysis.
Presentation/Outside Activities
- Does Renascience do any social activities?
-
As societies age rapidly, extending healthy life expectancy has become a critical global challenge. Through the research and development of pharmaceuticals and AI-driven medical technologies, we aim to contribute to a society where the elderly can lead healthy, independent lives.
We also actively promote open innovation in collaboration with universities, medical institutions, government bodies, and other companies, focusing on the practical application of research findings, the creation of medical innovations, talent development, and academic activities. We view contributing to a society of healthy longevity through these efforts as a key aspect of our Corporate Social Responsibility (CSR) and remain committed to disseminating research results and conducting public awareness activities.
- Please tell us about your latest academic activities.
-
□Lecture at the Tohoku University Discussion Meeting 2026: “Hagi no Yube” (The Challenge of Becoming the First Designated National University for International Excellence)
・February 27, 2026: Tohoku University Konwakai 2026 “Hagi no Yube” (Evening of Hagi)
Toshio Miyata, our Representative Director, Chairman, and President (also a professor at the Tohoku University Graduate School of Medicine), delivered a lecture at the “Hagi no Yube” (Evening of Hagi) event hosted by Tohoku University in 2026 (held at Marunouchi Building Hall). Speaking on the theme “Realizing a Longevity Society from Tohoku: Development of Longevity Pharmaceuticals,” he presented information on RS5614—a PAI-1 inhibitor and senolytic drug (a medication that eliminates senescent cells) currently under development by the company—highlighting its potential applications in anti-aging and longevity medicine, as well as our research and development efforts aimed at extending healthy life expectancy.□Lecture at the 6th MICHINOOK Seminar: “Industry-Academia Collaborative Life Sciences Tackling the Super-Aged Society—A Future Pioneered by Brain Science, Molecular Science, Drug Discovery, and AI”
・January 27, 2026 – 6th MICHINOOK Seminar: “Industry-Academia Collaboration in Life Sciences Tackling the Super-Aged Society”
Toshio Miyata, our Chairman and President (and Professor at the Tohoku University Graduate School of Medicine), delivered a lecture titled “Development of Senolytic Drugs” at the 6th MICHINOOK Seminar hosted by Tohoku University (held at Nihonbashi Life Science Hub). During the lecture, he discussed the potential of the PAI-1 inhibitor RS5614 as an anti-aging and longevity drug acting via the immune system, its clinical development status, and our participation in the international “XPRIZE Healthspan” project aimed at extending healthy lifespan.□Lecture at the “Life Science Innovation Forum 2025,” hosted by King Abdullah International Medical Research Center and J.P. Morgan Asset Management Co., Ltd.
・October 1, 2025: Life Science Innovation Forum 2025
Toshio Miyata—our Chairman and President (and a Professor at the Tohoku University Graduate School of Medicine)—was invited to the “Life Science Innovation Forum 2025” held in Riyadh, Saudi Arabia, where he delivered a presentation and participated in a panel discussion. He spoke about the roles of universities, research institutions, and startups in medical innovation, as well as the nature of international collaborative research, and introduced RS5614, a PAI-1 inhibitor currently under development by the company.
Development Pipeline
- What is important to increase the probability of success in drug development?
-
The important thing in drug development is to confirm safety and efficacy. Safety is carried out according to tests prescribed by pharmaceutical regulations, such as general toxicity and genotoxicity, so it can be done if there is time and funds. On the other hand, evaluating efficacy is not simple, and finding out which diseases a drug is effective against is a difficult task.
Developing a drug takes a lot of time and money. Even if it is not effective for the disease originally envisioned, it may be effective for another disease, so examining the efficacy of the drug for many diseases is important in increasing the probability of success (avoiding failure). It is difficult to broadly examine the indications of this drug (drug repositioning), and it is not realistic to examine it for all diseases.
We provide our developed compounds as “open resources” to researchers affiliated with public research institutes in Japan and overseas. Our framework, which allows us to collaborate with researchers in various fields engaged in cutting-edge basic research, allows us to conduct drug repositioning research far more efficiently and extensively than if we were to conduct basic research using only our own limited resources.
- What are the advantages of investigator-initiated clinical trials?
-
Our clinical trials are investigator-initiated trials conducted by physician scientists who are both researchers and doctors. The overwhelming advantages of investigator-initiated trials are their “quality” and “speed,” in other words, their “efficiency.”
In investigator-initiated clinical trials, doctors who are at the forefront of research and have access to the latest research results, and who treat patients on a daily basis in the medical field, can plan appropriate patient subjects and trial plans.
In addition, because doctors themselves can conduct clinical trials, this is a suitable framework for early-stage clinical trials of unapproved drugs (the stage where usefulness and safety are first confirmed, known as exploratory clinical trials). In addition, development of treatments for orphan diseases (rare diseases. Since the number of patients is small, not much sales can be expected) is not initiated by pharmaceutical companies due to low profitability, so in some cases, it is necessary to conduct investigator-initiated clinical trials from start to finish.
The vast majority of research and development costs are spent at the clinical development stage, not at the basic research stage. Investigator-initiated clinical trials can reduce development costs by quickly utilizing cutting-edge scientific and technological achievements from universities and other institutions, and by allowing clinical trial investigators to appropriately select patients who will be treated.
If we can find an appropriate coordinating physician and obtain support from multiple large medical institutions such as universities, investigator-initiated clinical trials have a significant advantage over corporate clinical trials, and large-scale clinical trials can be conducted in a short period of time, so unlike other companies, we prioritize this type of clinical trial.
- Is it possible to apply for regulatory approval with the results of investigator-initiated clinical trials?
-
In our pharmaceutical development, non-clinical trials are conducted in compliance with GLP (Good Laboratory Practice, standards for the implementation of pharmaceutical safety), and investigational drug manufacturing is conducted in compliance with GMP (Good Manufacturing Practice, standards for the manufacturing and quality control of investigational drugs).
In addition, investigator-initiated clinical trials, like corporate clinical trials, are conducted in compliance with Good Clinical Practice (GCP), which is a standard for conducting clinical trials of pharmaceuticals. Therefore, they can be used to apply for approval or obtain licenses.
- What are the reasons for the large number of drugs in your pipeline?
-
We provide the compounds we have developed as open resources to researchers affiliated with universities and other public research institutes both in Japan and overseas. By efficiently conducting a process known as drug repositioning to broaden the scope of indications for our drugs, we have succeeded in increasing our pipeline of numerous pharmaceutical products.
Compounds that are not candidates for clinical development are provided under a material transfer agreement (MTA), and clinical candidate compounds are provided under a collaborative research agreement (a contract that covers research licensing, intellectual property handling, and compensation after commercialization). Regarding our projects, the number of research institutions that have conducted research using compounds provided under MTA as open resources has reached over 100 since our founding, and these have been published in scientific papers alone. Unexpected seeds (concepts) have been born from these many domestic and international collaborative research projects.
- What kind of criteria do you have when deciding on pipeline development?
-
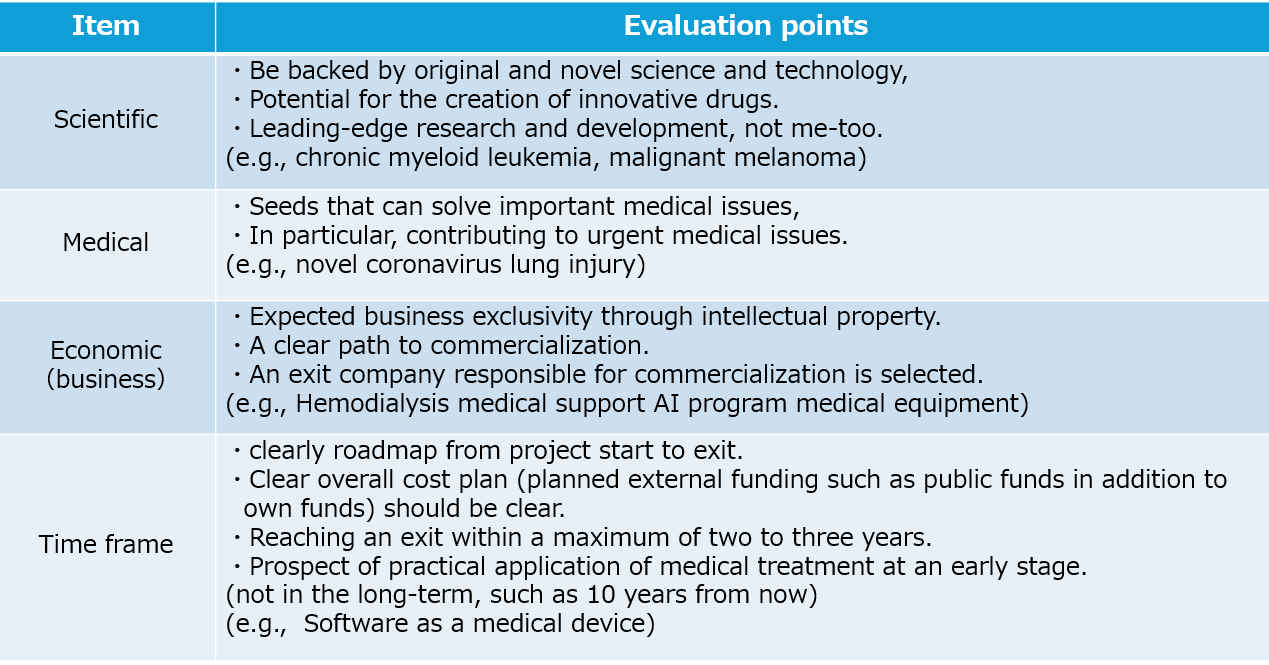
We make pipeline development decisions by comprehensively taking into consideration the four factors listed in the table below: “scientific viability,” “medical viability,” “economic viability (business viability),” and “time frame.”
- What are your considerations regarding intellectual property?
-
Since we conduct joint research with universities and other public research institutes, intellectual property is generally filed jointly with the universities, etc. In addition to complying with the regulations on inventions made during employment at universities, etc., we are required to hold repeated discussions with the university’s industry-academia collaboration department (intellectual property department) and to file, manage, and operate intellectual property in accordance with the university’s rules.
In addition, intellectual property applications are filed upon agreement on the inventors, applicants, ownership ratios of rights, cost burden, and even license conditions (scope, compensation), etc. These negotiations and agreements take a considerable amount of time (several months), so it is necessary to formulate an intellectual property application plan that takes this period into account.
Our intellectual property needs to be covered in Japan as well as in many other countries where we anticipate doing business. We also apply for, maintain, and manage multiple related intellectual property rights, such as substance patents, application patents, and dosage and administration patents, appropriately and continuously.
- What are the advantages in research and development of software as a medical device (SaMD) utilizing artificial intelligence (AI)?
-
The application of artificial intelligence (AI) to the medical field is a topic with great potential, but each of the stakeholders who play an important role in research and development is currently facing their own challenges.
Although doctors (medical institutions) are familiar with medical issues and problems (needs) and have a wealth of medical data and ideas, they lack AI methods and networks with IT vendors, and are therefore unable to concretely begin research and development.
On the other hand, although IT vendors with AI technology are interested in applying it to the promising medical field, it is not easy to put it into practical use due to the limited network with doctors (medical institutions) making it difficult to access medical needs and medical data, and the lack of experience in pharmaceutical administration, such as the Pharmaceuticals and Medical Devices Act.
Furthermore, pharmaceutical and health tech companies that want to commercialize the medical application of AI will often find it difficult to handle everything from research to business development on their own, both in terms of time and resources.
Therefore, it is important to have a framework in place from the beginning where doctors (medical institutions) with issues, IT vendors with AI technology, and pharmaceutical and health tech companies with the exit can work together to advance development. Because the product life cycle of programmed medical devices using AI is not as long as that of pharmaceuticals, efficient research and development requires planning from the early stages of development with an eye on approval and licensing and the exit into actual clinical practice.
To achieve this, open innovation across different fields is important, and in addition to doctors, data scientists, AI researchers, and pharmaceutical experts need to work together.
In the course of conducting many investigator-initiated clinical trials, we have built a network with numerous medical institutions and multiple medical departments. This gives us advantages such as easy access to medical issues and medical data (medical support), the ability to conclude joint research project agreements with multiple IT companies through open innovation (technical support), and the ability to comply with pharmaceutical regulations in the process of conducting investigator-initiated clinical trials for pharmaceuticals.
- What are the important aspects of medical applications of artificial intelligence (AI)?
-
The essential elements for research and development of medical AI are 1) medical issues, 2) medical data (quality and quantity), and 3) AI algorithms (engines).Even if there is excellent technology, there are many cases where it is difficult to put it into practical use because it does not match the needs of the medical field or there are issues with using it in the medical field, and this is a problem that many companies with technology face.
In recent years, a technique called “biodesign” has been gaining attention. It involves developing solutions based on the needs of medical professionals and then optimizing them while imagining the final product in the clinical setting. The same is true for programmed medical devices with AI as their core technology. While AI technology is certainly important, the medical data it develops is not targeted at machines but at patients, each with their own unique characteristics. Customizing AI based on medical issues, medical data, and the advice of medical professionals is crucial.
Medical data is an essential resource for AI research. While AI uncovers patterns from large amounts of data (inductive inference), a sufficient amount of data is undoubtedly necessary, data quality is just as important. Furthermore, the optimal AI algorithm must be selected based on the medical problem being solved and the type of medical data being utilized. Rather than searching for a medical field where a specific AI algorithm can be applied, it is necessary to “select (or, in some cases, develop) the optimal AI algorithm” to solve a specific medical problem. Furthermore, once an AI algorithm is selected, data scientists can use the data to analyze it, but only doctors can interpret and determine whether the results are correct. Therefore, without the involvement of doctors, it is impossible to train AI on high-quality medical data and solve problems.
Collaboration between doctors, data scientists, and AI researchers is important, and the active involvement of medical professionals (doctors) who have the medical issues, medical data, experience, and knowledge is key to successfully using AI to solve medical problems.
To promote research and development into the medical application of artificial intelligence, we signed a memorandum of understanding with NEC Solution Innovators, Ltd. in November 2022 and a joint research agreement (Memorandum of Understanding) with NEC Corporation in June 2023.
- How many pipelines are appropriate for the size of the company?
-
By providing our developed compounds as open resources to researchers affiliated with universities and other public research institutions both in Japan and overseas, we are able to efficiently explore the possibility of expanding the range of indications for our drugs within our limited resources (a process known as drug repositioning).
Because we do not require any in-house resources, there are no restrictions on the number of non-clinical trials (tests using disease animal models). Clinical development is conducted as investigator-initiated trials, utilizing contract research organizations (CROs), which reduces our in-house human resources.
We are steadily progressing with 10 clinical trials conducted in fiscal 2024, 9 in fiscal 2025, and 7 planned for fiscal 2026 (including one clinical performance study). Our goal is to continue conducting at least five investigator-initiated clinical trials per year.
- What pipeline is currently a high priority?
-
Pipeline development that is advanced in clinical development is a high priority.
Regarding pharmaceuticals, we are focusing on the development of plasminogen activator inhibitor-1 (PAI-1) inhibitors for oncology and respiratory indications. In the oncology field, Phase III trials are underway for chronic myeloid leukemia and malignant melanoma; a late-stage Phase II trial is in progress for non-small cell lung cancer; and a Phase II trial is being conducted for pancreatic cancer. Additionally, having completed a Phase II trial for cutaneous angiosarcoma with positive results, we are currently preparing for a Phase III trial. In the respiratory field, Phase II trials have been completed for COVID-19-induced lung injury and interstitial lung disease associated with systemic scleroderma.
Research and development for our medical device (an ultra-fine endoscope) is nearing completion; approval for the main fiber-optic scope unit was granted in December 2022, and development of the accessory guide catheter is essentially finished, so we plan to submit an application for regulatory approval during the fiscal year ending March 2027.
Regarding AI-based software as a medical device (SaMD), development is progressing on systems such as AI for diabetes treatment support and AI for maintenance hemodialysis support. Clinical performance trials for regulatory approval began in 2024; these trials have now been completed, and we have successfully established proof of concept (POC) for both the diabetes and dialysis applications.Regarding pharmaceuticals, we are focusing on the development of plasminogen activator inhibitor-1 (PAI-1) inhibitors for oncology and respiratory indications. In the oncology field, Phase III trials are underway for chronic myeloid leukemia and malignant melanoma; a late-stage Phase II trial is in progress for non-small cell lung cancer; and a Phase II trial is being conducted for pancreatic cancer. Additionally, having completed a Phase II trial for cutaneous angiosarcoma with positive results, we are currently preparing for a Phase III trial. In the respiratory field, Phase II trials have been completed for COVID-19-induced lung injury and interstitial lung disease associated with systemic scleroderma.
Research and development for our medical device (an ultra-fine endoscope) is nearing completion; approval for the main fiber-optic scope unit was granted in December 2022, and development of the accessory guide catheter is essentially finished, so we plan to submit an application for regulatory approval during the fiscal year ending March 2027.
Regarding AI-based software as a medical device (SaMD), development is progressing on systems such as AI for diabetes treatment support and AI for maintenance hemodialysis support. Clinical performance trials for regulatory approval began in 2024; these trials have now been completed, and we have successfully established proof of concept (POC) for both the diabetes and dialysis applications.
- What is the reason for developing the PAI-1 inhibitor in oncology?
-
Cancers with high PAI-1 expression are known to be highly aggressive and associated with a poor prognosis (the “PAI-1 paradox”). Through collaborative research, we discovered that PAI-1 promotes the expression of immune checkpoint molecules (such as PD-L1) on cancer cells. Studies using mouse models of colorectal cancer and malignant melanoma revealed that administration of our PAI-1 inhibitor reduced the expression of these immune checkpoint molecules on cancer cells, increased the infiltration of cytotoxic T cells into the tumor, and suppressed tumor-associated macrophages.
Based on these preclinical findings, we conducted a Phase II trial for malignant melanoma and confirmed the anticipated efficacy. When patients with malignant melanoma who were non-responsive to nivolumab were treated with a combination of nivolumab and RS5614 for eight weeks, an objective response rate (ORR) of 24.1% (7 out of 29 patients) was observed. This result exceeded the ORR associated with the existing combination therapy of nivolumab and ipilimumab (the ORR for the nivolumab and ipilimumab combination in Japan is 13.5%). Additionally, based on this concept, we conducted an investigator-initiated Phase II trial targeting non-small cell lung cancer. While no statistically significant difference was observed across the entire study population—which included patients receiving third-line therapy or later—an analysis of the 11 patients who received the study treatment as a third-line therapy showed high efficacy, with an ORR of 18.2% and a 6-month progression-free survival rate of 27.5%. These results confirm that the PAI-1 paradox plays a role in cancer treatment and that the use of PAI-1 inhibitors in combination therapy is effective for certain types of cancer.
- How was the PAI-1 inhibitor obtained?
-
Based on the crystal structure of the human PAI-1 molecule, we used computational engineering to search a virtual compound library of approximately 2 million compounds and identified 96 PAI-1 inhibitor candidate compounds. Using PAI-1 inhibitory activity as an indicator, we have synthesized over 1,400 new inhibitor compounds over the course of more than 10 years. After screening for efficacy and evaluating their safety and efficacy, we identified RS5275, an orally bioavailable lead compound with excellent safety. Further synthesis of RS5275 yielded four clinical candidate compounds: RS5441, RS5484, RS5509, and RS5614. RS5614 was ultimately selected as the candidate compound for clinical development.
- How is the status of domestic and international competition for PAI-1 inhibitor development?
-
In the past, many pharmaceutical companies and biotech ventures, including major ones both in Japan and overseas, have worked on developing small molecule PAI-1 inhibitors. Some drugs have been reported to be effective in animal models of mice and rats, and PAI-749 (Diaplasinin) even made it to the clinical stage. However, no effect was observed in humans, and development was discontinued after Phase I clinical trials.
- Are there any safety issues with the PAI-1 inhibitor?
-
Non-clinical studies have included safety pharmacology studies (hERG studies, rat central nervous system studies, monkey cardiovascular and respiratory system studies), general toxicity studies (a 26-week oral administration study in rats, and a 39-week oral administration study in monkeys), genotoxicity studies, phototoxicity studies, and reproductive and developmental toxicity studies to confirm that there are no issues for clinical trials or regulatory approval applications.
A Phase I single-dose study confirmed the safety of RS5614 up to 240 mg, and a Phase I repeated-dose study observed mild adverse events following oral administration of 120 mg for seven days. RS5614 has been administered to over 200 subjects (healthy individuals, patients with chronic myeloid leukemia, patients with COVID-19 lung injury, and patients with melanoma, among others). In a 48-week study of patients with chronic myeloid leukemia, 180 mg daily was administered (33 cases). No serious adverse events related to the investigational drug have been reported, and the drug is considered to be highly safe.
- What is the reason for developing the PAI-1 inhibitor in chronic myeloid leukemia (CML)?
-
CML, a type of blood cancer, develops when chromosomal abnormalities occur in hematopoietic stem cells, leading to the uncontrolled proliferation of cancerous leukemia cells (CML cells).
The mainstay of treatment for CML is the tyrosine kinase inhibitor TKI (such as imatinib). However, while TKIs act on CML cells, they do not affect CML stem cells, which reside in bone marrow niches and are the source of CML. Therefore, discontinuing TKI treatment allows CML cells to proliferate, preventing a complete cure of CML. It has been shown that PAI-1 inhibitors act on CML stem cells, enhancing the action of TKIs, thereby leading to a complete cure of CML. In fact, when RS5614 was administered in combination with a TKI in CML model mice, the number of CML stem cells remaining in the bone marrow was significantly reduced compared to administration of the TKI alone, significantly improving survival rates.
Although the development of TKIs has significantly improved the prognosis for CML patients, long-term, expensive TKI treatment is required to cure CML. Side effects from long-term continuous use are also a problem. Therefore, it is important to achieve a cure (treatment-free remission, TFR) that does not require TKI use as soon as possible. RS5614 is expected to be a safe drug with a new mechanism of action that will quickly lead many CML patients to TFR.
- What were the results of the Phase II trial for chronic myeloid leukemia (CML)?
-
In the Phase IIa trial, CML patients who had been receiving TKI treatment for at least two years were administered RS5614 120 mg/day for four weeks (TKI treatment continued for 12 weeks). The investigator-initiated trial was conducted at Tohoku University, Akita University, and Tokai University, and the rate of DMR (deep molecular response: highest therapeutic effect) achieved after 12 weeks was used as an indicator. 21 patients were enrolled, and there were no dropouts or discontinuations, so all were included in the analysis. The primary endpoint was that four of the 21 patients achieved DMR, with a cumulative DMR rate at 12 weeks of 20.0% (the average cumulative DMR rate at three months with previous TKI monotherapy was 2.0% (treatment with TKI alone was referred to as the historical control)). In the safety evaluation, no side effects were observed in any of the 21 patients included in the analysis.
In the Phase IIb study, CML patients were administered a combination of a TKI and RS5614 (starting at 150 mg/day, with the option to increase to 180 mg/day), with the objectives of confirming that a cumulative DMR achievement rate of 33.0% could be expected 48 weeks after the start of RS5614 administration, compared to 8.0% in historical controls, and of confirming the pharmacokinetics and safety of RS5614 when administered long-term in combination with a TKI. Of the 33 patients, 11 achieved a DMR, with a cumulative DMR achievement rate of 33.3% at 48 weeks (a result equal to or better than expected (POC)). Regarding safety, there were no serious adverse events causally related to the investigational drug.
- Please tell us about the Phase III trial for chronic myeloid leukemia (CML).
-
Based on the results of the late Phase II study, a placebo-controlled, double-blind, investigator-initiated Phase III clinical trial to evaluate the efficacy of the combination of TKI and RS5614 in patients with chronic phase CML is underway in collaboration with 12 universities and medical institutions, including Tohoku University, Tokai University, and Akita University. This study was adopted by the Japan Agency for Medical Research and Development (AMED) under the Research Program of the “Practical Application for Innovative Cancer Therapy” in fiscal 2022 (Tohoku University is the representative research organization and Renascience participates as a sharing research organization). In November and December 2021, we held face-to-face consultations with the Pharmaceuticals and Medical Devices Agency (PMDA), and in May 2022, we submitted a notification of the clinical trial plan to the PMDA and started a multicenter Phase III study. Sixty (60) patients with chronic stage CML who had been treated with TKI for more than 3 years will be enrolled in the study, and the study will evaluate whether the combination of RS5614 significantly increases the maintenance rate of DMR for more than 2 years compared to TKI alone in 60 patients with chronic CML who have been treated with TKI for more than 3 years.
- What is the reason for developing the PAI-1 inhibitor in malignant melanoma?
-
Currently, there are four major cancer treatments: 1) surgery, 2) radiation therapy, 3) chemotherapy (anticancer drugs), and 4) immunotherapy. Of these, immunotherapy utilizes the body’s natural immune system to attack cancer. Various immunotherapies have been proposed, but the most effective are immune checkpoint inhibitors, which inhibit the immune brakes. Because excessive immune responses are harmful, the body has mechanisms to suppress them. The molecules that perform this brake function are called immune checkpoint molecules. In fact, cancer exploits these immune checkpoint molecules to prevent its own immune system from working against itself.
Immune checkpoint inhibitors inhibit immune checkpoint molecules, thereby releasing these brakes and activating the immune response against cancer. We have discovered that PAI-1 inhibits cancer immunity via immune checkpoint molecules. In animal model studies, it was found that cancers such as malignant melanoma and colon cancer regressed in animals administered RS5614, and that when administered in combination with an immune checkpoint inhibitor antibody, it strongly synergistically enhanced cancer immunity.
The immune checkpoint inhibitory effects of the PAI-1 inhibitor RS5614 were confirmed in a Phase II trial of malignant melanoma.
(What is malignant melanoma?)
Malignant melanoma is a type of skin cancer that develops when melanocytes, the skin cells that produce melanin, the pigment responsible for skin color, become malignant. It has a high metastasis rate and is considered highly malignant among skin cancers. While the number of melanoma patients in Japan is low, at 1.5-2 per 100,000, the rate in the United States is 21.0, several dozen times higher than in Japan. Malignant melanoma is an extremely malignant cancer (the 5-year survival rate is approximately 50% for tumors over 4 mm in size, approximately 40% for those with regional lymph node metastasis, and several percent for those with distant metastasis). Furthermore, it has been reported that the progression rate of malignant melanoma in Japan is approximately three times higher than in the United States. This is because malignant melanoma in Japan is often of the acral lentigo type, which differs from that in Europe and the United States and is thought to make treatment less effective.
Treatment for malignant melanoma begins with surgical removal. However, in many cases, cancer is already advanced at the time of detection, and in cases where radical resection is not possible, chemotherapy (drugs) is required. Radiation therapy is not very effective for malignant melanoma. The introduction of antibody drugs (immune checkpoint inhibitors) such as nivolumab that target immune checkpoint molecules has led to groundbreaking advances in chemotherapy. However, the response rate of nivolumab for malignant melanoma in Japan is only 22.2%. Furthermore, for patients in whom nivolumab is ineffective, combination therapy with nivolumab and ipilimumab has been approved, but the response rate is 21% overseas and 13.5% in Japan. Nivolumab-ipilimumab combination therapy causes severe side effects in over half of patients, and the incidence of severe immune-related side effects leading to treatment discontinuation is four times higher than with monotherapy, resulting in months of hospitalization and interruption of cancer treatment. Furthermore, given the high medical costs, there is a strong need for a combination drug that uses a different modality from antibodies, can be administered orally, has fewer side effects, and increases response rates.
- Please tell us the results of the Phase II trial for malignant melanoma.
-
A Phase II investigator-initiated clinical trial was conducted in collaboration with six medical institutions, including Tohoku University Hospital, to investigate the efficacy and safety of combining the PAI-1 inhibitor RS5614 with the immune checkpoint inhibitor nivolumab in patients with malignant melanoma that is difficult to completely resect surgically. The results showed that the combination of nivolumab and RS5614 was equally or more effective than the reported combination of nivolumab and ipilimumab, an existing treatment (response rate of 24.1% for nivolumab + RS5614, 13.5% for nivolumab + ipilimumab). Furthermore, while there are safety concerns regarding the combination of nivolumab and ipilimumab due to serious immune-related side effects, no problematic side effects were observed with the combination of nivolumab and RS5614.
Results of a Phase II Investigator-Initiated Clinical Trial
Efficacy
・The primary efficacy endpoint, the response rate after 8 weeks of concomitant use of RS5614, was 24.1%.
・The disease control rate (complete response (CR) + partial response (PR) + stable disease (SD)) was 62.0%.
Safety
・Of the 34 patients included in the safety analysis, 11 serious adverse events occurred in 9 patients by 8 weeks of treatment, with 2 cases of liver dysfunction (5.9%) possibly related to the study drug.
- How will RS5614 change the treatment of malignant melanoma?
-
Currently, in melanoma, insurance coverage is available for the combination of nivolumab and ipilimumab in patients who are resistant to nivolumab, but serious side effects associated with the nivolumab-ipilimumab combination have become a problem. The Japan Clinical Oncology Group (JCOG) began a Phase III trial (JCOG2007 trial) at 59 facilities nationwide in April 2021 to compare the efficacy of nivolumab + ipilimumab combination therapy in patients with non-small cell lung cancer. However, the trial was discontinued on March 30, 2023, due to an unexpectedly high treatment-related death rate of approximately 7.4% (11 out of 148 patients) in the nivolumab-ipilimumab combination group. Thus, the combination of nivolumab and ipilimumab presents problems regardless of the type of cancer.
In a Phase II trial targeting malignant melanoma, the combination of RS5614 and nivolumab demonstrated equal or greater efficacy than the combination of nivolumab and ipilimumab in patients for whom nivolumab was ineffective, and the combination of nivolumab and RS5614 demonstrated greater safety than the combination of nivolumab and ipilimumab. Based on the above, the development of a new treatment for unresectable malignant melanoma for which immune checkpoint inhibitor monotherapy is ineffective is an urgent issue, and the combination of nivolumab and RS5614 is expected to be a drug therapy with high efficacy and safety.
- Is RS5614 useful in the treatment of other solid tumors?
-
Non-clinical studies using animal models have shown that oral administration of the PAI-1 inhibitor RS5614 can cause regression of not only malignant melanoma, but also other cancers such as colorectal cancer and lung cancer, and that this effect is significantly enhanced when combined with immune checkpoint inhibitor antibodies. Therefore, we conducted a Phase II investigator-initiated clinical trial for non-small cell lung cancer and a Phase II investigator-initiated clinical trial for cutaneous angiosarcoma in collaboration with Hiroshima University Hospital and other medical institutions. As a result, we have confirmed efficacy in angiosarcoma and non-small cell lung cancer. Currently, a late-stage Phase II trial is underway for non-small cell lung cancer, while preparations for a Phase III trial are proceeding for angiosarcoma.
- What is the medical significance of the clinical trial for malignant melanoma?
-
It has previously been reported that cancers with high PAI-1 expression are highly malignant and have poor prognoses, a phenomenon known as the “PAI-1 paradox.” Through collaborative research with numerous universities both in Japan and abroad, we have discovered that cancer cells evade attack from the immune system by producing PAI-1 and enhancing the expression of immune checkpoint molecules such as PD-L1. In preclinical studies using animal models, we have demonstrated that oral administration of the PAI-1 inhibitor RS5614 can cause regression of melanoma, colon cancer, lung cancer, and other cancers. In this clinical trial, we administered RS5614 for eight weeks in combination with 29 melanoma patients for whom surgical resection was difficult and for whom nivolumab was ineffective. Seven patients responded to RS5614. RS5614 has already been demonstrated to be effective as a drug therapy for chronic myeloid leukemia, a type of blood cancer, in Phase II trials (early and late phases), and Phase III trials are currently underway. These findings demonstrate that the “PAI-1 paradox” is indeed important in cancer treatment, that PAI-1 is a therapeutic target for some types of cancer, and that PAI-1 inhibitors are effective as drug therapy in humans.
- Please tell me about the Phase III trial for melanoma.
-
Based on the results of the Phase II trial, we are currently conducting a Phase III randomized, placebo-controlled, double-blind, investigator-initiated clinical trial in collaboration with 18 universities and medical institutions, including Tohoku University, Sapporo Medical University, and Kumamoto University, to evaluate the efficacy and safety of combining nivolumab with RS5614 in 124 patients with unresectable melanoma. This trial was selected for the National Institutes of Biomedical Innovation, Health, and Nutrition’s FY2025 “Orphan Drug Research Grant Program.”
The trial was approved by the Institutional Review Board (IRB) at Tohoku University Hospital in January 2025, and the Phase III trial began in February 2025, with the first dose administered. This trial will evaluate whether the combination of nivolumab with the investigational drug RS5614 significantly extends survival compared to the nivolumab monotherapy group in 124 patients with unresectable melanoma.
- When will RS5614 be available for use in the medical field as a treatment for malignant melanoma?
-
We were able to confirm its efficacy in a Phase II trial. We will continue discussions with regulatory authorities and, depending on the results of the Phase III trial currently underway, will clarify our future roadmap, including approval applications. Furthermore, as we do not hold a pharmaceutical manufacturing and sales license, we hope to clarify the path to commercialization through collaboration with other companies.
- What is the difference between RS5614, a PAI-1 inhibitor, and other immune checkpoint inhibitors?
-
All immune checkpoint inhibitors to date are antibody drugs that require hospitalization and administration by injection, making them expensive. Furthermore, existing antibody drugs are known to have various side effects. RS5614 is highly safe and is expected to be an oral medication that can be taken at home. Furthermore, unlike antibodies, it is produced by chemical synthesis, so its price is expected to be lower than that of antibodies.
- What is the reason for developing the PAI-1 inhibitor in lung cancer?
-
Standard treatment for non-small cell lung cancer is platinum-based chemotherapy and immunotherapy using anti-PD-1/PD-L1 antibodies, but few cases are curative. In cases where this treatment is ineffective, chemotherapy such as docetaxel is administered as second-line treatment, but survival times are short at three months, necessitating third-line treatment. Effective third-line treatments are scarce, and new therapeutic agents are eagerly awaited.
Through collaborative research, we have discovered that PAI-1 is involved in the progression and proliferation of lung cancer, and confirmed that cancer cells resistant to anti-PD-1 antibodies express extremely high levels of PAI-1. In fact, in a non-clinical study using a lung cancer model mouse, we confirmed that combined administration of an anti-PD-1 antibody and a PAI-1 inhibitor demonstrated greater anti-cancer activity than administration of an anti-PD-1 antibody alone.
Based on these findings, a Phase II trial was conducted to evaluate the combination therapy of nivolumab and RS5614 in patients with unresectable advanced or recurrent non-small cell lung cancer who had previously received multiple lines of anticancer drug therapy. The results showed an objective response rate of 18.2% and a 6-month progression-free survival rate of 27.5% in patients receiving third-line treatment; this demonstrated superior antitumor efficacy compared to nivolumab monotherapy, with no new safety concerns identified. Building on these results, an investigator-initiated Phase II trial is currently underway for patients with locally advanced non-small cell lung cancer, evaluating the addition of RS5614 to the standard first-line treatment regimen of chemoradiotherapy followed by consolidation therapy with durvalumab.
- What is the reason for developing the PAI-1 inhibitor in cutaneous angiosarcoma?
-
Cutaneous angiosarcoma is a rare soft tissue tumor (approximately 300 cases per year in Japan), and apoptosis-inducing taxane anticancer drugs are the first-line treatment. However, a prognosis study of 90 cases of cutaneous angiosarcoma treated with taxane anticancer drugs found that the overall survival rate was 649 days, indicating limited therapeutic benefit. Research and development of new therapeutic agents is urgently needed. PAI-1 is primarily produced in the vascular endothelium.
In our analysis of cutaneous angiosarcoma samples, we found that high PAI-1 expression strongly correlates with disease prognosis. The finding that cancer cells with high PAI-1 expression are resistant to apoptosis strongly suggests that the combined use of a PAI-1 inhibitor may enhance the therapeutic efficacy of taxane anticancer drugs in angiosarcoma. Consequently, a Phase II trial (investigator-initiated clinical trial) was conducted at Tohoku University and other institutions, targeting patients with cutaneous angiosarcoma who had become refractory to the taxane-based anticancer drug paclitaxel. The results showed a progression-free survival (PFS) of 4.0 months and an overall survival (OS) of 20.8 months—outperforming existing treatments—with disease stabilization confirmed in 13 out of 15 patients (86.7%); furthermore, no serious or previously unknown adverse events were observed. Based on these findings, preparations are currently underway for the next phase of the trial and for practical implementation.
*Apoptosis: A phenomenon in which a cell’s own death program is activated, leading to cell death, as opposed to necrosis , in which cells die due to injury.
- Is the PAI-1 inhibitor effective in preventing aging?
-
In collaboration with Northwestern University in the United States, we have conducted research on “PAI-1 and aging.”
Living cells cannot proliferate indefinitely due to a phenomenon known as cellular senescence. This phenomenon is caused by shortening of gene telomere length and cellular senescence factors such as p53. It is known that senescent cells express extremely high levels of PAI-1 in addition to p53. In fact, it has been shown that cellular senescence can be inhibited by suppressing p53 and PAI-1. It has been reported that PAI-1 expression is high not only in cells, but also in aged tissues and individuals (klotho mice, and humans with Werner syndrome, a well-known premature aging disorder). In klotho mice, a well-known aging model, we have shown that inhibiting PAI-1 expression and activity at the gene or protein level can improve all of the cardinal symptoms of aging.
Furthermore, a study of members of the Amish community, a Christian sect living in the Midwestern United States, found that those without the PAI-1 gene lived 10 years longer than those with it. The researchers also found that those with the gene deficiency were less susceptible to diseases such as diabetes.
These findings were reported in numerous newspapers, including the New York Times in November 2017. The lead researcher, a professor at Northwestern University, stated, “Not only are they living longer, but they are also living healthier lives. They are the ideal longevity model.” This human epidemiological study is consistent with the results of cell and mouse experiments. With aging, diseases such as cancer, vascular (atherosclerosis), lung (emphysema, chronic obstructive pulmonary disease), metabolism (diabetes, obesity), kidney (chronic kidney disease), bone and joint (osteoporosis, osteoarthritis), and brain (cerebrovascular disease, Alzheimer’s disease, dementia) develop. Interestingly, PAI-1 expression is extremely high in tissues associated with these diseases. Furthermore, it has been confirmed that administering PAI-1 inhibitors to animal models of these diseases significantly improves their pathology.
Recently, it has been shown that senescent cells express proteins (immune checkpoint molecules) that act as brakes on the immune system, allowing them to escape immune attack. When aging mice or mice with lifestyle-related diseases are administered drugs that block immune checkpoint molecules (immune checkpoint inhibitors), the immune system is activated, removing senescent cells and improving organ and tissue aging and lifestyle-related diseases. We have discovered that PAI-1 is involved in the expression of immune checkpoint molecules in cancer cells, promoting cancer cell proliferation, and that PAI-1 inhibitors have immune checkpoint inhibitory effects. Thus, PAI-1 promotes cancer and aging, and our PAI-1 inhibitors are expected to be effective against cancer and other aging-related diseases.
In conclusion, fascinating insights are emerging regarding PAI-1 and aging.
Furthermore, as a semi-finalist (Top 40) in the “XPRIZE Healthspan”—an international competition aimed at extending healthspan—we conducted a semi-final clinical trial of RS5614. The results demonstrated that a four-month administration period rejuvenated biological age (epigenetic age) by an average of two to three years. Additionally, the findings suggested systemic anti-aging effects, including improvements in biomarkers related to immune, bone/muscle, metabolic, and cognitive functions; the recovery of hematopoietic stem cell function; and a reduction in oxidative stress. A generally favorable safety profile was also confirmed. We remain committed to advancing research and development aimed at extending healthspan.
- What is XPRIZE Healthspan?
-
It is a global competition offering a total prize purse of $100 million USD to research teams that succeed in extending healthspan. Organized by the XPRIZE Foundation, the initiative aims to revolutionize therapeutic approaches to human aging and longevity by tackling the ambitious challenge of actively extending healthspan by more than ten years. ( https://www.xprize.org/prizes/healthspan )
- Why develop nucleic acid drugs?
-
Our company is researching and developing medical solutions using various modalities to solve medical challenges, and we are conducting investigator-initiated clinical trials for multiple pipelines. Luxana Biotech, our collaborative research partner in nucleic acid drugs, is researching and developing highly effective and safe biopharmaceuticals (nucleic acid drugs) using a drug discovery platform technology utilizing artificially modified nucleic acids developed by Professor Satoshi Kobiga of the Graduate School of Pharmaceutical Sciences at Osaka University. Therefore, we have decided to jointly conduct research, clinical development, and commercialization of novel nucleic acid drugs, leveraging Luxana Biotech’s artificially modified nucleic acid technology and our track record and experience in investigator-initiated clinical trials.
This research has been selected for the Japan Agency for Medical Research and Development (AMED)’s “Smart Bio Drug Discovery Research Support Project” (Osaka University is the lead research institution, and our company is a contributing research institution) in fiscal year 2024.
- What is SaMD utilizing AI for diagnosis of swallowing dysfunction?
-
If left untreated, age-related decline in oral function (called oral frailty) can lead to numerous physical and social disabilities, such as eating disorders and speech disorders, as well as generalized muscle weakness (frailty). Therefore, early diagnosis and appropriate treatment are important. Dysphagia, a type of oral function decline, is on the rise in an aging society, and it has been reported that approximately 70% of pneumonia deaths are caused by aspiration. Early detection of swallowing dysfunction and therapeutic interventions such as rehabilitation are important to prevent aspiration pneumonia. However, currently, the only swallowing assessment methods available are swallowing endoscopy and swallowing fluoroscopy, which place a significant burden on patients.
Since the organs used in swallowing and speech share many common parts, such as the tongue, oral cavity, and pharynx, we are focusing on the possibility of evaluating swallowing function from speech. We are developing AI that can evaluate swallowing dysfunction from speech data during conversation. In collaboration with several departments at Tohoku University (Otolaryngology, Dentistry, and Rehabilitation Department, School of Biomedical Engineering) and NEC Corporation, we have developed an AI system that analyzes the full frequency range of speech from patients visiting the Tohoku University Hospital Swallowing Treatment Center using an AI engine specialized in time-series data analysis (time-series model-free analysis). This system confirms the baseline of healthy subjects’ speech (gender, age, individual differences, etc.), detects differences between healthy subjects’ pronunciation and that of patients, and diagnoses swallowing dysfunction.
We will continue to train the system on data from elderly people with swallowing dysfunction and move toward practical application. If this program medical device is put into practical use, it is expected to enable easy and early diagnosis of patients with swallowing dysfunction who may develop aspiration pneumonia.
- What other projects are you working on to develop SaMD utilizing AI?
-
As part of our efforts in women’s diseases, one of our priority areas, we are jointly developing AI with Tohoku University to detect lesions from breast cancer pathology images. In testing using pathology images, we classified the detection model into three classes (benign, non-invasive cancer, invasive cancer) or two classes (benign, malignant), achieving diagnostic accuracy of 88.3% and 90.5%, respectively. Furthermore, we developed an AI system for breast cancer detection using frozen pathological sections during intraoperative rapid diagnosis, achieving a diagnostic accuracy of 92.3% for benign versus malignant classification, and 89.2% when further classifying cases into non-invasive and invasive cancer. These results have been published in an academic paper.
In addition, as part of our efforts in aging-related diseases, we are jointly developing AI with Tohoku University to predict the occurrence of arrhythmias and heart failure using information from cardiac implantable devices.
Furthermore, in September 2022, we signed a joint research agreement with Hi-Lex Corporation and Hi-Lex Medical Co., Ltd., and are working with Hi-Lex Medical Co., Ltd. and Tohoku University to develop AI to predict the occurrence of thrombosis in ventricular assist devices.
- What is important in the development of a medical device and software as a medical device?
-
Even with excellent technology, there are many cases where medical application (practical use) is difficult because the technology does not match the challenges and needs of the medical field or is inappropriate for the specifications of the medical field, and many companies with technology face this problem. Our company develops solutions to problems starting from the needs of the medical field, and develops optimized products by imagining the final product in the medical field, striving to develop medical devices and programmed medical devices based on the idea of “biodesign,” which realizes innovation.
Financials
- How were your full-year results for the fiscal year ending March 31, 2026?
-
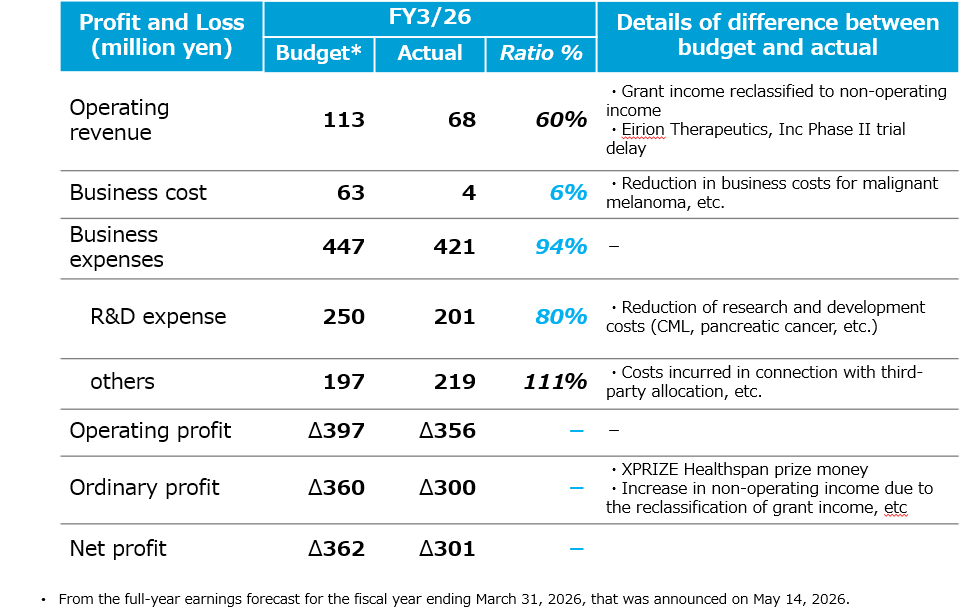
For the full year ending March 2026, operating revenue was 68 million yen, operating loss was 356 million yen, ordinary loss was 300 million yen, and net loss was 301 million yen. Although business revenue decreased compared to the previous fiscal year, milestone income related to the development of AI-equipped hemodialysis medical devices with Toray Medical Co., Ltd. and products utilizing AI algorithms to predict optimal fluid volume for chronic dialysis patients with Nipro Co., Ltd. We have recorded the initial contract payment, the initial contract payment from the extension of the joint development agreement, and contract research income related to the AMED business.
Compared to the plan, business revenue increased by 60%, mainly due to grants from the National Research and Development Agency, National Research and Development Agency for Biomedical Innovation, Health and Nutrition This was due to changes in revenue display categories (to non-operating income) and delays in starting Phase II trials by Allion. On the other hand, contest prize money and grant income from placing in the XPRIZE Healthspan TOP40 (semifinalists) were recorded as non-operating income.
In terms of costs, compared to the plan, the reduction in business costs related to malignant melanoma and the efficiency of research and development expenses related to CML and pancreatic cancer resulted in project expenses totaling 421 million yen (compared to the plan). 94%), and research and development expenses amounted to 201 million yen (80% of the plan). While efficiently utilizing limited management resources, we continuously promote the development of multiple pipelines including CML, malignant melanoma, non-small cell lung cancer, cutaneous angiosarcoma, pancreatic cancer, and anti-aging and longevity-related research.
As a result, operating losses amounted to 356 million yen, reducing the planned loss of 397 million yen. Furthermore, by recording 36 million yen in prize money from the XPRIZE Healthspan contest and 27 million yen in grants from the National Research and Development Agency for Biomedical Innovation, Health and Nutrition Research and local governments, the operating loss was 300 million yen, Net loss for the period was 301 million yen, indicating a significant improvement in profitability on a profit basis compared to the plan.
- When do you announce your financial results?
-
First quarter: around mid-August, second quarter: around mid-November, third quarter: around mid-February, financial results announcement: around mid-May.
Please see the following page.
- Do you have a timeline for turning to profitability at this point?
-
While it is difficult to specify exactly when we will achieve consistent profitability, we aim to reach this long-term goal by actively leveraging public research grants and generating revenue through the out-licensing of our pipeline—including upfront payments, milestone payments linked to development stages, and royalties based on product sales.
Stock/Shareholder
- What is the status of your major shareholders?
-
Please see the following page.
- Who should I contact for IR inquiries?
-
We will post frequently asked questions in the FAQ section of our website.