News
Notice of Publication of the Result of Late Phase II Study for Chronic Myeloid Leukemia
We are pleased to announce that the result of our late phase II study of RS5614 (PAI-1 inhibitor) for chronic myeloid leukemia (“CML”) is published in a peer-reviewed scientific journal “Cancer Medicine”.
Takahashi N, Kameoka Y, Onizuka M, Onishi Y, Takahashi F, Dan T, Miyata T, Ando K, Harigae H. Deep molecular response in patients with chronic phase chronic myeloid leukemia treated with the plasminogen activator inhibitor-1 inhibitor TM5614 (*1) combined with a tyrosine kinase inhibitor. Cancer Medicine. 2022 online. (http://doi.org/10.1002/cam4.5292)
CML is caused by an abnormality (genetic mutation), the formation of BCR-ABL gene that exhibits tyrosine kinase activity, in the chromosomes of hematopoietic stem cells (*2), which leads to the unrestricted growth of cancerous leukemia cells. The mainstay of treatment is molecular targeted drugs (tyrosine kinase inhibitors (*3), “TKIs”) such as imatinib. A major problem in the treatment of CML is that patients who experience long-term remission by treatment with TKIs often relapse when the drugs are withdrawn.
The CML patients increase every year, due to its high incidence in the elderly population in an aging society and the decrease in mortality rates resulting from advances in TKIs therapy.
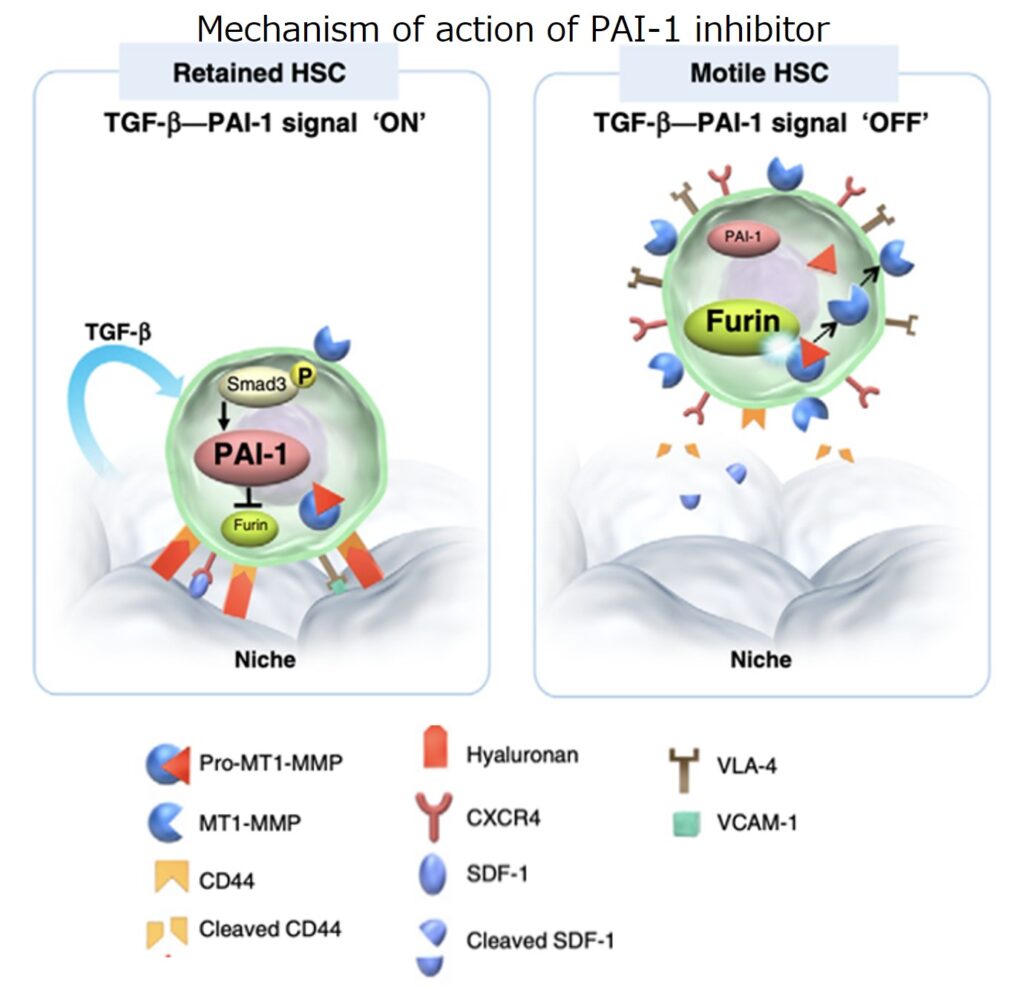
Hematopoietic stem cells reside in the bone marrow niche (*4), where PAI-1 is highly expressed intracellularly in the milieu of abundant tumor growth factor-β (*5). PAI-1 can bind to and inhibit the intracellular enzyme furin (*6) in hematopoietic stem cells. The PAI-1 inhibitor RS5614 blocks the binding of intracellular PAI-1 to furin and then activates membrane-type matrix metalloproteinases (*7), thereby promoting mobilization of the hematopoietic stem cells from the bone marrow niche.
The reason why CML relapses after TKIs withdrawal is because TKIs do not act on cancerous hematopoietic stem cells (cancer stem cells) hiding in the bone marrow niche. A collaborative study with Tokai University strongly suggests that the PAI-1 inhibitor RS5614 can liberate cancer stem cells from the bone marrow niche and enhance the action of TKIs, thereby leading to complete cure of CML (Yahata T, Ibrahim AA, Hirano K, Muguruma Y, Naka K, Hozumi K, Vaughan DE, Miyata T, Ando K. Targeting of plasminogen activator inhibitor-1 activity promotes elimination of chronic myeloid leukemia stem cells. Haematologica. 2021; 106: 483).
Continuous therapy with expensive TKIs for as long as 30 years or more is required to cure CML, and it causes a significant medical economic burden. Side effects by long-term use of TKIs have also become a problem, which include deaths due to myocardial infarction or stroke, and blindness due to retinal artery occlusion. Therefore, it is important to achieve a complete cure that does not require TKIs as early as possible. Recently, it became evident that CML patients who have been in deep molecular remission (*8) (“DMR”; MR4.5, the amount of the cancer-causing gene BCR-ACL IS is less than 0.0032%), for a certain period can be cured without molecular relapse after TKIs discontinuation. However, only 8-12% of the CML patients can be cured with TKIs in the shortest treatment period of three years. RS5614 is a safe drug candidate with a novel mechanism of action that can cure many CML patients at an early stage.
In a late phase II study of TKIs plus RS5614 in patients with chronic CML, the cumulative DMR rate was 33.3% at 48 weeks after treatment with TKIs plus RS5614, compared to 8% after 48 weeks of treatment with TKIs alone. Thus, we have obtained a proof-of-concept (that is the confirmation of the therapeutic efficacy). Furthermore, the safety of RS5614 was confirmed since there were no serious adverse events causally related to the drug.
We have initiated a phase III trial for CML, as announced on August 3, 2022. We would like to make this drug available for CML patients as early as possible.
(*1) TM5614: Clinical Development Number of RS5614 (PAI-1 inhibitor)
(*2) Hematopoietic stem cells: Stem cells that can differentiate into blood cells
(*3) Tyrosine kinase inhibitor: Tyrosine kinase is a type of protein kinase that adds phosphate to tyrosine, one of the amino acids that make up proteins, and plays an important role in transmitting signals related to cell growth and differentiation. When a tyrosine kinase is abnormally activated by genetic mutation, cells proliferate abnormally and cause diseases such as cancer. A tyrosine kinase inhibitor specifically inhibits a tyrosine kinase.
(*4) Bone marrow niche: Hematopoietic stem cells are maintained in a quiescent state by a special environment called a “niche” in the bone marrow to prevent them from dividing in vain to keep their ability to self-renew when needed and to prevent the aging and loss of function.
(*5) Tumor growth factor-β : A cytokine (a type of secreted protein that regulates cell functions) that controls cell growth and differentiation, and promotes cell death.
(*6) Furin: A major protein-processing enzyme in the protein secretory pathway of cells. It cleaves various proteins at a specific sequence.
(*7) Membrane-type matrix metalloproteinase: A proteolytic enzyme localized on the cell surface that degrades extracellular substrates. It retains zinc ions in its active center.
(*8) Deep molecular remission: The amount of the BCR/ABL gene that causes CML is measured by molecular genetic methods. If the amount of the gene drops below 0.0032% for two consecutive measurements after treatment, the patient is defined in deep molecular remission (“DMR”).